When you’re taking a proton pump inhibitor (PPI) like omeprazole for heartburn and also need an antifungal like itraconazole for a stubborn fungal infection, something unexpected can happen: the antifungal stops working as well as it should. This isn’t a myth or a guess-it’s a well-documented, clinically significant interaction that’s been studied for over 30 years. And it’s more common than you think. About 39% of patients prescribed itraconazole capsules also get a PPI at the same time, according to Medicare data from 2022. That’s nearly four in ten people whose treatment could be failing without anyone realizing why.
Why PPIs Kill Antifungal Absorption
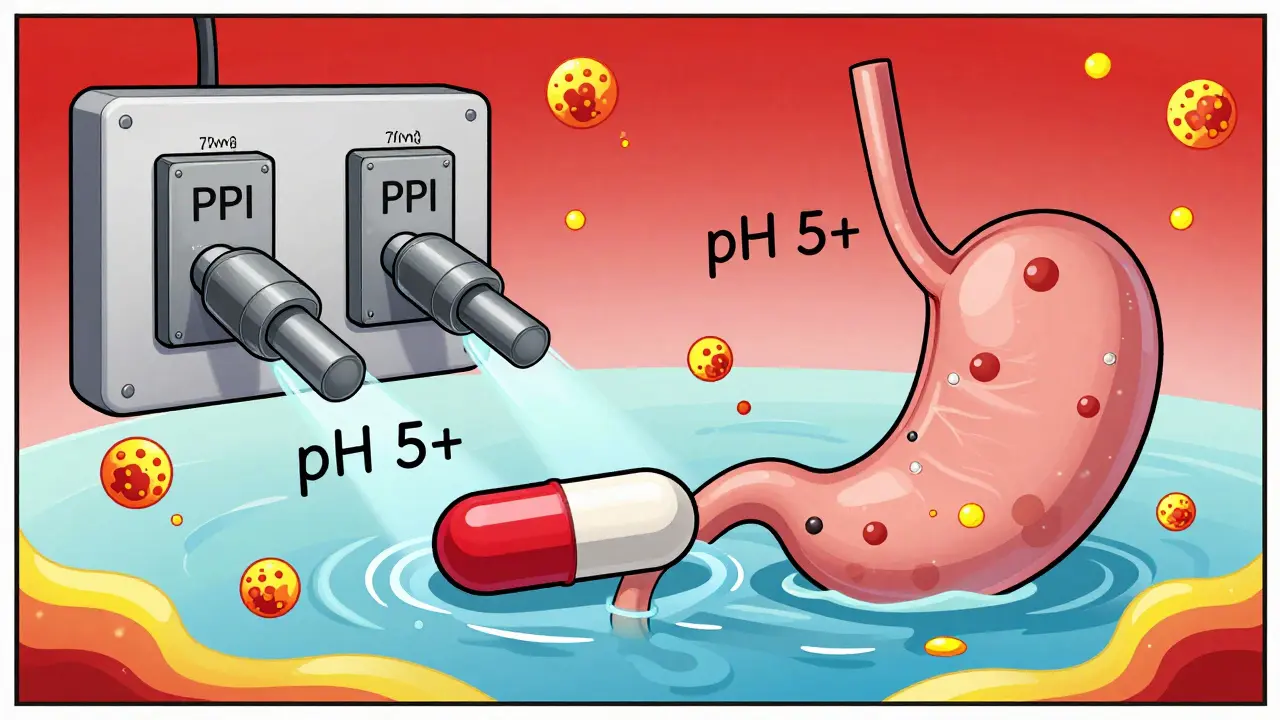
PPIs work by shutting down the acid pumps in your stomach. That’s great if you have GERD. But it’s a problem for certain antifungals because they need acid to dissolve properly. Think of it like this: some antifungal pills are designed to break down only in a highly acidic environment-like itraconazole capsules. When you take a PPI, your stomach pH rises from around 1.5 to 5 or higher. At that pH, itraconazole doesn’t dissolve. It just sits there, unchanged, and passes through your gut without being absorbed. Studies show this isn’t minor. When you take itraconazole capsules with a PPI, your blood levels of the drug can drop by 50% to 60%. That’s not a small dip-it’s enough to push your drug concentration below the level needed to kill fungi. In one JAMA Network Open study, patients on both drugs had 60% less itraconazole in their bloodstream over 24 hours. That’s the difference between a treatment that works and one that doesn’t.Not All Antifungals Are Affected the Same
This interaction doesn’t apply to every antifungal. Fluconazole, for example, is highly water-soluble and doesn’t need stomach acid to be absorbed. Its levels stay steady whether you’re on omeprazole or not. Voriconazole is somewhere in the middle-its absorption drops by about 22% with PPIs, but it’s still often usable with careful dosing. Posaconazole is tricky: the delayed-release tablet loses 40% of its absorption with PPIs, but the oral suspension doesn’t drop nearly as much. The real problem is with itraconazole capsules. They’re the most common form prescribed, and they’re the most vulnerable. But there’s a solution: the itraconazole solution (liquid form). It’s already dissolved, so it doesn’t rely on stomach acid. Studies show it only loses 10-15% of absorption when taken with a PPI. That’s why, in hospitals, pharmacists often switch patients from capsules to solution when PPIs can’t be stopped.What About Other Acid Reducers?
H2 blockers like famotidine (Pepcid) or ranitidine also reduce stomach acid-but not as much or as long as PPIs. PPIs suppress acid for up to 24 hours. H2 blockers last 4 to 10 hours. That makes a big difference. One study found omeprazole reduced itraconazole absorption by 57%, while famotidine only cut it by 41%. That’s still a problem, but it’s less severe. Antacids? They’re different. They neutralize acid temporarily, but don’t block its production. If you take an antacid two hours before or after your antifungal, it usually won’t interfere. The key is timing. But antacids aren’t a long-term solution for chronic acid reflux-they’re meant for occasional use.
Real Patients, Real Consequences
This isn’t just theory. Hospital pharmacists report seeing this interaction every month. A 2022 survey of over 1,200 pharmacists found 68% had encountered at least one case of treatment failure due to this interaction. One case from Massachusetts General Hospital involved a patient with chronic pulmonary aspergillosis. His itraconazole blood levels were at 0.3 mcg/mL-far below the 0.5 mcg/mL minimum needed. His doctor switched him from omeprazole to famotidine. Within two weeks, his levels jumped to 1.7 mcg/mL. He stopped having lung flare-ups. Another patient, treated at MD Anderson, had invasive aspergillosis and needed both voriconazole and omeprazole. Instead of stopping the PPI, the team gave the antifungal two hours before the PPI. That small change kept the drug levels in range. No treatment failure. No hospital readmission. These aren’t rare exceptions. They’re routine fixes that work when people know to look for the problem.What Should You Do?
If you’re on a PPI and your doctor prescribes itraconazole capsules, ask: Is there a better option? The solution form of itraconazole is just as effective and doesn’t need acid to work. If you can’t switch, ask if you can temporarily stop the PPI. For many patients with mild reflux, a two-week break from PPIs during antifungal treatment is safe. If you can’t stop the PPI, here’s what works:- Switch from itraconazole capsules to itraconazole solution
- Use famotidine instead of a PPI, and take it at least 10 hours after the antifungal
- Take voriconazole or posaconazole suspension instead of tablets
- For posaconazole tablets, take them with a cola drink-it lowers the pH in the stomach and helps absorption
- Never take itraconazole capsules with a PPI at the same time
Therapeutic Drug Monitoring Is Key
For serious infections like invasive aspergillosis, doctors should check blood levels of itraconazole. The target range is 0.5 to 1.0 mcg/mL. If you’re on a PPI and your level is below 0.5, it’s not because the drug isn’t strong enough-it’s because your stomach isn’t acidic enough. Adjusting the acid suppression can fix it. Pharmacists are the unsung heroes here. Studies show that when pharmacists actively manage these interactions-by reviewing med lists, recommending alternatives, and educating patients-82% of patients get the right care. Without that intervention, treatment failure rates jump.
9 Comments
OMG I CANNOT BELIEVE THIS ISN’T COMMON KNOWLEDGE 😭 My aunt took omeprazole and itraconazole and her fungal nail thing got WORSE for 8 months-doc just kept prescribing more pills like it was her fault. I had to drag her to a pharmacist who actually knew what was going on. Why do doctors not teach this???
It’s wild how such a simple physiological mechanism-acid-dependent dissolution-gets ignored in practice. We’ve got AI diagnosing skin rashes, but we still miss drug interactions that have been documented since the 90s. It’s not a lack of knowledge, it’s a system failure. The fact that pharmacists are the ones catching this 82% of the time says everything about how fragmented care has become.
bro i was just telling my cousin this last week-he’s on omeprazole for ‘stress stomach’ and got prescribed itraconazole for athlete’s foot. he thought it was ‘just a pill’ and didn’t even ask. now he’s got a fungal infection that won’t quit. i’m not a doctor but i googled it and now i’m the family pharmacist 😅
It is imperative that healthcare professionals recognize the clinical significance of this pharmacokinetic interaction. The bioavailability compromise of itraconazole capsules in the presence of proton pump inhibitors is not merely a theoretical concern-it represents a tangible, quantifiable deviation from therapeutic thresholds, thereby compromising patient outcomes and increasing healthcare expenditures. Institutions must implement mandatory pharmacist-led medication reconciliation protocols to mitigate this preventable failure.
THIS IS WHY BIG PHARMA WANTS YOU ON PPIs FOREVER. They know if you stop the acid blocker, your heartburn goes away-so they make the antifungals useless so you gotta keep buying more pills. The FDA knows. Doctors know. But they’re too busy getting paid by the drug companies. Tolsura? That’s just a fancy name for ‘we finally fixed our own mess.’
From a pharmacokinetic standpoint, the pH-dependent solubility of azole antifungals is a textbook example of formulation-driven bioavailability constraints. Itraconazole’s logP and pKa profile render it critically dependent on gastric acidification for dissolution-unlike fluconazole, which is zwitterionic and water-soluble across physiological pH. The 50–60% AUC reduction with PPIs is consistent with first-pass absorption kinetics. The solution formulation bypasses this entirely via pre-dissolution, making it the gold standard in polypharmacy scenarios. Tolsura’s pH-independent absorption profile represents a paradigm shift in solid dosage design.
USA is falling apart. In my day, doctors didn’t hand out PPIs like candy. Now we got people on omeprazole since 2012 for ‘indigestion’ and wonder why their fungus won’t go away. Fix your diet, stop eating junk, and stop letting Big Pharma turn your stomach into a neutral swamp. Also, why are we using Indian doctors to fix American medical mistakes? Just saying.
While the data presented is statistically significant, it lacks longitudinal follow-up. The 68% pharmacist-reported case incidence is anecdotal and unvalidated by controlled trials. Furthermore, the assertion that ‘stopping PPIs is safe for mild reflux’ is clinically reckless-GERD progression to Barrett’s esophagus is not trivial. Without stratified risk assessment, recommending PPI discontinuation is irresponsible.
So let me get this straight… we’re spending $287 million a year because doctors are too lazy to read the label? I’m just here for the drama.
Write a comment